
Countries, laws and news
Our never-ending #BlackProtest
Read stories from Polish women on reproductive rights in the book #MyBlackProtest and discover the creation of a worldwide feminist movement.
Facing an unplanned pregnancy, exploring contraception options, or needing abortion care?
Our blog is here to empower you with all the information and support you need! Dive into our easy-to-read articles on safe abortion, discover real stories from people like you, and get the latest tips and advice from experts on the best uses of the abortion pills, Mifepristone and Misoprostol. Whether you're looking for answers or just need some medical abortion guidance, our blog has everything to help you make the best choices and feel confident on your journey.

Dive into easy-to-read articles on safe abortion, and get the latest tips and advice from experts.
Read stories from Polish women on reproductive rights in the book #MyBlackProtest and discover the creation of a worldwide feminist movement.
Explore the considerations for deciding when it's safe and emotionally comfortable to have sex after an abortion. Learn more here.
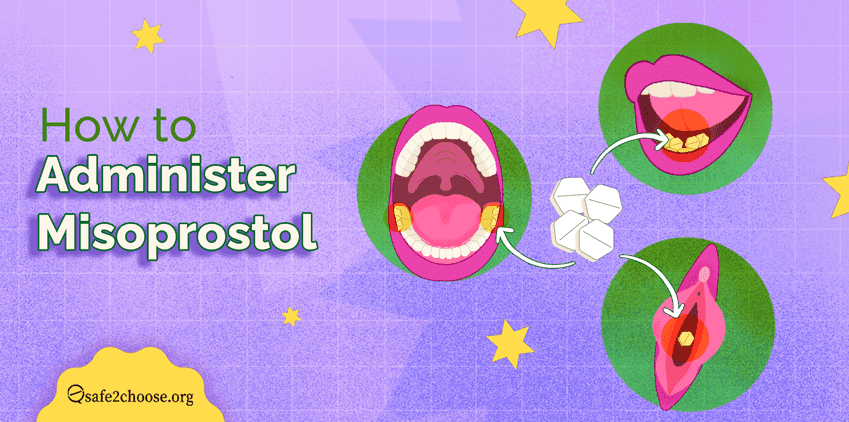
Get comprehensive guidance on how to properly administer Misoprostol and what to expect during the process. Ensure a safe experience.
Learn about abortion in Kenya: legal status, safe methods (pills & procedures), costs, and barriers to access. Find accurate guidance here.

Learn what ovulation is, when it happens, common signs, and why it’s important for pregnancy, fertility, and reproductive health.
Medical abortion allows you to terminate a pregnancy using two pills (mifepristone and misoprostol) check here the preparations, and the risks

Learn how abortions performed with Mifepristone result in shorter waiting times and the possibility to have abortions at home without surgery.

Discover what reproductive health really means, beyond biology. Learn how it protects your body, rights, and future.
Discover how long HCG levels remain in the body after an abortion and when to expect a negative pregnancy test. Learn about it here on safe2choose

Learn about the signs of pregnancy after an abortion, including warning signs of infection or womb damage, and what to do if you experience any symptoms.

Worried about vomiting after taking the abortion pill? Learn when it matters, and what to do next to ensure a safe and effective abortion.
Explore how Miss World Philippines 2025 empowers women by advocating for reproductive health, family planning, and informed choice

Explore the different types of contraceptives, understand family planning, and learn how to make safe decisions. Find support here.

We talk about ectopic pregnancy, including its symptoms, causes, risk factors, treatments, & emotional recovery. Know when to seek help here.

Learn the common symptoms after an abortion with pills and know when to seek help. Get expert guidance for a safe and smooth recovery.
View 1 - 15 of 100
CONTACT US
If you need more information or didn't find what you were looking for, don't hesitate to contact us through our counseling page and communication channels.

